IN THIS ARTICLE
DISCHARGE INSTRUCTIONS WALLET INFO-CARD When to call your doctor
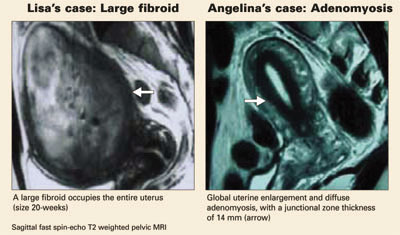
LISA’S CASE
Ablation fails to ease symptoms
Lisa is a 38-year-old mother of 2 who initially reported menometrorrhagia, dysmenorrhea, urinary frequency, pelvic pressure, and increasing abdominal girth. These symptoms worsened over 3 years before Lisa saw a physician and was diagnosed with uterine fibroids. When offered hysterectomy or endometrial ablation (cryomyolysis), she chose the latter. However, her fibroids failed to shrink, and her symptoms returned 5 months after the procedure.
Lisa heard about uterine artery embolization (UAE) through the media and now asks about it. Her uterus is 20-week size with an irregular contour. Magnetic resonance imaging (MRI) shows a single large fibroid filling the uterus. Her hematocrit is 22.
Is uterine UAE right for her?
ANGELINA’S CASE
Menorrhagia and a “boggy” uterus
Angelina, 35, has 2 children and a 10-year history of menorrhagia, dysmenorrhea, and anemia. Pelvic examination reveals a 10-week size, “boggy” uterus, and MRI shows global enlargement of the uterus with a thickened junctional zone, which is characteristic of adenomyosis.
Her previous physician recommended hysterectomy after medical therapy failed, but Angelina is reluctant to undergo surgery.
Is UAE an option?
Both women are very likely to benefit from UAE, since the ideal candidate is premenopausal with symptomatic fibroids and/or adenomyosis and has either failed medical or surgical therapy or wants or needs to avoid surgery.1-11
This article describes the therapeutic role of UAE in women with abnormal uterine bleeding (AUB) due to uterine fibroids and/or adenomyosis—the most frequent myometrial causes of premenopausal AUB.
Other, less frequent myometrial disorders (eg, hypervascular pathologies such as intramyometrial and parametrial vascular malformations or neoplasms) can also be treated using embolization techniques. The main advantages of UAE in treating these diseases:1-8,12,13
- Less invasive than surgery, with substantially less recovery time and lower morbidity
- Usually performed under local anesthesia and intravenous conscious sedation
- No worry about adhesions
- Virtually no blood loss or need for transfusion; UAE may be especially attractive for patients who refuse or cannot receive blood products for health or religious reasons.
Impressive success rates
UAE has demonstrated excellent technical (98% to 100%) and high clinical success rates (80% to 95%) in the treatment of fibroids.1-8,13 The clinical success rate is lower for adenomyosis (56% to 92%), but UAE often provides sufficient clinical relief to obviate surgery.9,10,13
Although UAE was not initially recommended for women desiring future fertility—because of the 4% risk of premature menopause—the pendulum is now swinging in the other direction. If the risks of myomectomy are great due to the anatomic size or position of fibroids or adenomyosis, the risk-benefit ratio may shift to UAE to allow preservation of reproductive capacity.1-8,11
Though embolization has been performed since the early 1970s for acute and chronic bleeding associated with various medical conditions,14 the first report of UAE did not come until 1995.1 Since then, the procedure has seen rapid growth worldwide, with approximately 50,000 cases performed. About 14,000 cases were performed in the US last year.2
Although our practice has no fixed size limitation, ideally a uterus less than 20 weeks’ gestational size is preferred.
Contraindications
- Viable pregnancy
- Active pelvic infection
- Presence of an intrauterine device (though the IUD may be removed before the rocedure)
- Undiagnosed pelvic or adnexal mass
- Pelvic malignancies such as ovarian or endometrial carcinoma
- History of pelvic radiation, since UAE may cause ischemic necrosis of the uterus and adjacent organs due to preexisting radiation-induced vasculitis with diffuse vascular narrowing.
Relative contraindications
- Renal insufficiency, though we have used gadolinium, a nonnephrotoxic MRI contrast medium, for women with high blood creatinine levels
- History of severe allergic reaction to iodinated contrast medium, though gadolinium can also be used in these patients
- Coagulopathy
- Desire to preserve fertility, since it cannot be assured based on current data. However, uncomplicated pregnancies and normal deliveries have been reported after UAE, so this procedure may still be preferred for women who refuse or cannot undergo myomectomy.11