
Obstetric hemorrhage is a major cause of maternal death worldwide. Clinical research conducted in major trauma units shows that mortality can be reduced by:
- developing and practicing standardized processes for responding to massive hemorrhage
- defining, beforehand, the transfusion approach to massive hemorrhage—the so-called massive transfusion protocol, or MTP.
Take a look at California’s OB hemorrhage guideline
Leaders in obstetrics in California have developed and released a guideline for managing massive obstetric hemorrhage and improving outcomes that involves four ascending stages of response1:
Stage 0. Assess women for risk factors for hemorrhage. Actively manage the third stage of labor by administering oxytocin and performing fundal massage.
Stage 1. Activate the hemorrhage protocol when blood loss exceeds what would be considered a normal volume. Immediately:
- assemble appropriate personnel (head nurse, anesthesiologist, additional obstetricians if available)
- establish large-bore intravenous access
- increase the rate of oxytocin infusion
- perform fundal massage
- administer methergine (if the mother is not hypertensive)
- prepare to transfuse 2 units of packed red blood cells (RBCs).
Stage 2. If bleeding continues, assemble the OB rapid response team. Also:
- assess coagulation status
- administer additional uterotonic agents, such as misoprostol and carboprost tromethamine (Hemabate)
- move to an operating room
- consider dilation and curettage
- place an intrauterine balloon
- consider interventional radiology and uterine artery embolization
- consider laparotomy and either uterine compression stitches or hysterectomy.
Stage 3. If bleeding persists and exceeds a predetermined volume:
- activate the MTP
- mobilize additional gyn surgical resources and an additional anesthesiologist
- repeat all laboratory tests
- perform laparotomy and consider hysterectomy.
(Note: This guideline for managing OB hemorrhage is summarized in the California Maternal Quality Care Collaborative’s TABLE.)
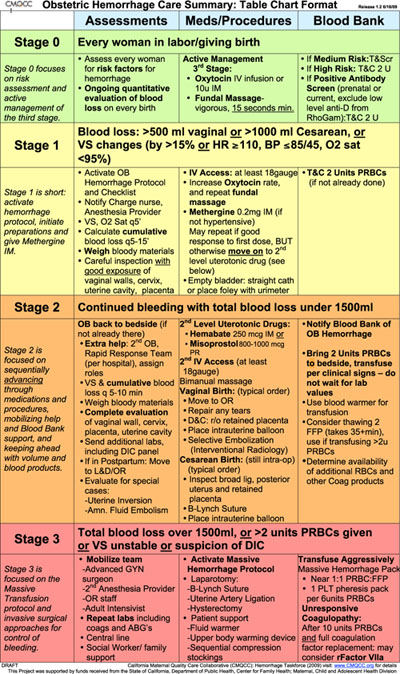
Obstetric Hemorrhage Care Summary: Table Chart Format
A massive transfusion protocol is invaluable
Evidence from trauma centers demonstrates that an MTP reduces the risk of death and morbidity from major hemorrhage.2-5 MTPs vary by center, but their common feature is rapid delivery of multiple units of blood, fresh frozen plasma (FFP), and platelets to the operating room (OR) where the mother has been brought.
It’s not an exaggeration to say that, in the past, a clinician managing a massive bleed had to beg the blood bank to release adequate blood products. In the new MTP approach, the blood bank sends a standardized amount of products to the OR immediately after the MTP is triggered.
The MTP at Brigham and Women’s Hospital. Our MTP calls for 2 units of RBCs and 2 units of FFP to be delivered by pneumatic tube within a few minutes. Additional products—4 more units of RBCs and 2 more units each of FFP and platelets—are delivered shortly thereafter.
There are alternatives: For example, an MTP can call for 6 units of RBCs, 4 units of FFP, and 6 units of platelets to be sent to the OR.
MTPs also emphasize the standardized transfusion ratio of units of RBCs to FFP of roughly 1:1, or 2:1 until coagulation status can be adequately assessed. Some MTPs also define the ratio of units of RBCs to platelets that should be utilized—for example, 5:1.
Common coagulation targets of MTPs are:
- hematocrit, ≥21%
- international normalized ratio (INR), ≤1.5
- platelets, ≥50K/μL
- fibrinogen, ≥100 mg/dL.
Trauma centers have more experience with MTPs, but major obstetric units have also discovered that they help clinicians and patients.6
RiaSTAP to the rescue for small OB units?
Many smaller obstetric hospitals do not have adequate blood products immediately available to deal with massive OB hemorrhage. In many cases of OB hemorrhage, all endogenous fibrinogen is consumed, and a key to saving the life of the mother is to replace fibrinogen rapidly.
Recently, the FDA approved a lyophilized fibrinogen concentrate (RiaSTAP) for congenital hypofibrinogenemia. Although RiaSTAP is expensive, it is stable and could be stocked by the blood bank of a small hospital for (off-label) use in massive hemorrhage.
Unlike cryoprecipitate, a commonly used source of fibrinogen that can take 30 minutes or longer to thaw, RiaSTAP can be quickly reconstituted with sterile water.
RiaSTAP might be apppropriate when it would take longer than 30 minutes to thaw cryoprecipitate and fibrinogen infusion is needed sooner. Combining RiaSTAP with FFP would provide most of the critical proteins in the coagulation cascade.
Saving lives worldwide with a balloon catheter
The intrauterine balloon is now widely recognized as a simple intervention that can often resolve massive OB bleeding.7,8 Two FDA-approved intrauterine balloons are available:
- the Bakri Postpartum Balloon (Cook Medical)
- the BT-Cath (Utah Medical Products).
The Bakri Postpartum Balloon has been widely utilized; clinicians should be familiar with its use. I discussed this device in my February 2009 Editorial.