
Key points
- In a 1998 Kaiser review, 52% of high-grade lesions were preceded by either a smear of ASCUS or AGUS.
- The most common histologic abnormality found is ASCUS, not AGUS.
- Under the 2001 Bethesda System, atypical squamous cells are subclassified into ASC-US (undetermined significance) and ASC-H (cannot exclude high-grade dysplasia.)
With the newest iteration of the Bethesda System in place—the second revision in 10 years—the clinician is again asked to learn new classifications of cervical cytology and the attendant management protocols. One purpose of the new system is to eliminate the confusion and variability of the previous Papanicolaou (Pap) Class II smear and the CIN Class 2R smear, both of which acted as “hedges” to let the clinician decide on management.1
Under the newest system, atypical squamous cells are subclassified into ASC-US (undetermined significance) and ASC-H (cannot exclude high-grade dysplasia). Atypical glandular cells of undetermined significance (AGUS) also have been subclassified. The reason: To create specific readings of cell changes, as atypical cells often are seen prior to dysplasia. In fact, in a 1998 Kaiser review, 52% of high-grade lesions were preceded by either a smear of ASCUS or atypical glandular cells of undetermined significant (AGUS). The most frequent precursor smear was ASCUS (43.6%).2
While the terminology has been tightened, cytologic laboratories still lack uniformity in their reporting of atypical cells. When reviewed by consulting cytopathologists, a significant percentage of these smears are reclassified as normal. But, since clinical management decisions are based on the original cytology, there is the possibility of both false-negative and false-positive Pap test results. Consequently, patients are either subjected to more active management or a delay in diagnosing a serious abnormality.
Add managed care to the equation, and more difficulties arise. Currently, it is unusual for a gynecologist to choose his or her cytologic laboratory or pathologist. Instead, these designations are frequently determined by the patient’s insurance company, reducing a clinician’s ability to consult with a cytopathologist with whom he or she is acquainted. Despite these obstacles, the recent FDA approval of liquidbased cytology and human Papillomavirus (HPV) testing has helped to augment patient care and management. With these new technologies and others on the way, it is important to understand the management algorithms available. Following are my preferences in evaluating and treating patients with either ASCUS or AGUS cytology.
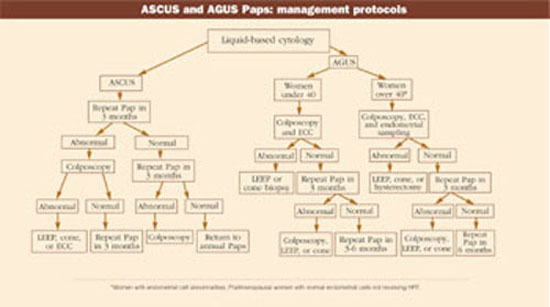
Managing ASCUS
Use liquid-based cytology for those patients who have ASCUS or AGUS smears or any cellular abnormality including previous dysplasia; a clinically abnormal cervix; or a history of postcoital bleeding; and/or heavy vaginal discharge. While this collection method can be used in the presence of a small amount of menstrual blood, do not take the smear if there is normal or heavy menstrual bleeding. Collect the specimen using either a spatula and endobrush or cytobrush (paint brush).
Perform a repeat Pap smear in 3 months in patients who have ASC-US cytology but no previous abnormal history. I do not treat nonspecific inflammation. Perform a colposcopy when a second ASC-US smear is reported. If the colposcopy is satisfactory and no abnormality is seen, do not perform an endocervical curettage (ECC) or cervical biopsy. Repeat the Pap smear in 6 months. (Bear in mind that follow-up smears should be negative at least twice before returning the patient to the usual cycle of yearly Paps.) When colposcopy is unsatisfactory, an ECC is indicated. If the ECC is negative, the patient is followed by a repeat smear in 6 months. Administering vaginal estrogen may be helpful in the postmenopausal patient, as it promotes epithelial maturation since immature cells may be confused with atypical squamous cells.
On the other hand, when ASC-H is found, schedule an immediate colposcopy. In addition, colposcope all patients who are considered at high risk for cervical cancer, including women with HIV or renal transplants.3
Managing AGUS
AGUS is another borderline classification. Although the subclassifications have been reduced from the previous Bethesda System (refer to www.bethesda2001.cancer.gov for a complete breakdown of the subclassifications), there are still management decisions that have to be made. Fortunately, the most common histologic abnormality found is ASCUS, not AGUS.4 Furthermore, lesions associated with AGUS are usually found near the external os, not high in the endocervix. Colposcopically, subtle changes in endocervical glandular cells may represent normal metaplasia, atypical metaplasia, microglandular hyperplasia, intraepithelial neoplasia, or even early invasive adenocarcinoma.5 Therefore, clinicians are obligated to sample more tissue sites.
In contrast to ASCUS, neither observation nor a repeat Pap smear is an option because the potential for abnormalities is much higher in the AGUS smear. Management is based on the AGUS subclassification (if given) and the patient’s age.