<huc>A</huc> Perhaps. Women treated for subclinical infection had significantly fewer preterm births than controls, Kiss et al found. However, I am not yet ready to embrace routine screening of all gravidas for asymptomatic candidiasis, trichomoniasis, and bacterial vaginosis (BV), though I strongly recommend treating symptomatic infections.
Expert Commentary
Before you embrace the screening program recommended by Kiss et al, be aware that their observations are inconsistent with other published reports and with our understanding of the pathophysiology of preterm delivery related to genital tract infection.
In this prospective, randomized trial, more than 4,000 asymptomatic gravidas were screened for vaginal candidiasis, trichomoniasis, and BV. When infection was detected, the intervention group was treated and the control group was not. The frequency of preterm birth was 3.0% in the intervention group (P=.0001) and 5.3% in the control group. The intervention group also had significantly fewer infants weighing less than 2,500 g.
How the findings contradict other data
I question these findings due to the following:
- To my knowledge, the study is unique in suggesting an association between vaginal candidiasis and preterm delivery.
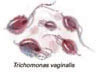
- In a large multicenter US study,1 treating gravidas with asymptomatic trichomoniasis did not prevent preterm delivery. In fact, treated women had a higher frequency of preterm delivery (19.0% versus 10.7%, P=.004).
- In another large multicenter US study,2 treating asymptomatic BV did not reduce the frequency of preterm delivery or other adverse outcomes.

The regimens Kiss et al used for trichomoniasis and BV are not standard in the United States. They administered topical metronidazole to treat trichomoniasis and topical clindamycin for BV. The current recommendation for treating trichomoniasis in pregnancy is a single 2-g oral dose of metronidazole.3 For BV, recommended treatment is oral metronidazole, 250 mg three times daily for 7 days.3
Systemic regimens are based on the hypothesis that organisms ascend from the lower genital tract through the endocervical canal and colonize the membranes, causing inflammation and activating the prostaglandin cascade. Presumably, topical vaginal therapy will not eradicate organisms colonizing the upper genital tract.

These results may not be widely applicable, since the women treated by Kiss et al were extremely low-risk. Ninety-eight percent of the women were white, and the total prevalence of the 3 vaginal infections was only 20%. In many US sectors, the prevalence of BV alone exceeds 30%. Unfortunately, based on results of the studies cited above, I do not believe US obstetricians should anticipate the favorable results noted by Kiss et al.