CASE Could bowel obstruction have been prevented?
B.H., 34, undergoes laparotomy for removal of an 8-cm myoma and a left ovarian cyst, which is found to be an endometrioma. Now she has come to the emergency department complaining of abdominal distension, pain, vomiting, and an inability to defecate. Small-bowel obstruction is diagnosed. Another laparotomy reveals that the obstructed bowel is adhered to the prior surgical incision.
Could this scenario have been avoided?
Adhesions need no introduction. Every surgeon is familiar with them; they are so ubiquitous they sometimes seem to be a given. Nevertheless, there are steps you can take to reduce the incidence of postoperative adhesions. In this article we describe surgical techniques, barriers, and peritoneal instillates that can help.
Why worry?
Intra-abdominal adhesions can cause pain, infertility, and bowel obstruction, and complicate future surgeries.1-3 Most studies suggest that more than 50% of women with adhesion-related small bowel obstruction have a history of gynecologic or obstetric operations. Within 1 year of laparotomy, adhesions cause intestinal obstruction in 1% of patients. After even a single previous abdominal operation, 93% of patients develop adhesions, compared with only 10.4% of patients who have never undergone laparotomy (FIGURE 1).1-3
We recently found an incidence of adhesion-related intestinal obstruction after operation for a benign gynecologic indication of 8 cases per 1,000 operations.4 Total abdominal hysterectomy (TAH) was the most common cause of small bowel obstruction (13.6 cases per 1,000 surgeries).
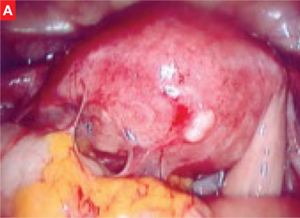
FIGURE 1 Adhesions through the laparoscope
Severe adhesions between the intestines and omentum to the uterus.
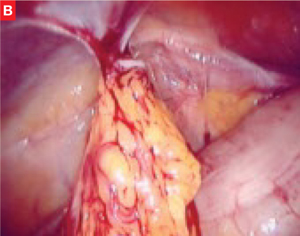
Omental adhesions to the anterior abdominal wall.
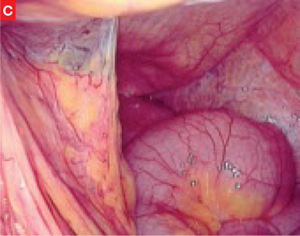
Adhesion between the intestine (lower left hand corner) and the anterior abdominal wall.
Surgical technique
Basic strategies
Tissue desiccation, necrosis, and the use of reactive suture material can predispose the patient to adhesion formation. Many studies in animal models have demonstrated an association between adhesions and these parameters. The following practices can help:
- Continuously irrigate the operative field during laparotomy
- Use nonreactive suture material such as polyglycolic acid (Dexon), polyglactin (Vicryl), or polydioxanone (PDS). Using reactive material, such as catgut, is discouraged
- Use powder-free gloves and prevent foreign-body infiltration (eg, powder, gauze, lint) of the wound.
No single parameter is as important as good surgical technique, attention to microsurgical principles, and precise hemostasis (TABLE 1).
TABLE 1
Surgical principles to reduce adhesion formation
| Take a laparoscopic approach when feasible |
| Minimize tissue necrosis |
| Provide meticulous hemostasis |
| Liberally irrigate the abdominal cavity |
| Use nonreactive suture materials |
When performing laparotomy
|
Peritoneal closure is unnecessary
Several randomized trials have demonstrated that closure of the parietal or visceral peritoneum is unnecessary. This practice is associated with slightly longer operating times and greater postoperative pain and may cause more adhesions.5 In 1 study, the rate of adhesion formation after laparotomy with peritoneal closure was 22.2%, compared with 16% without closure.6
Ellis7 noted an increasing number of medicolegal claims arising from adhesion-related complications, and recommended that “peritoneal defects and the pelvic floor should be left open, since they rapidly reperitonealized.”
Laparoscopy is more protective than open surgery
Abdominal surgeries injure tissues more severely than laparoscopy, and are associated with a greater degree of adhesion formation in up to 94% of patients, although laparoscopy can also cause adhesions.2 Laparoscopy is more protective because it involves minimal handling of tissue and little manipulation of the internal organs. Surgery is performed in a closed environment, tissue moistness is maintained, and contamination with glove powders or lint does not occur. In addition, the tamponade effect of carbon dioxide pneumoperitoneum facilitates hemostasis. Laparoscopy is also associated with a lower incidence of infection.
Adhesion-reducing substances
Many adhesion-reducing products have been evaluated in human and animal models. A basic assumption behind these substances is that surgically injured tissues heal without forming adhesions if the traumatized surfaces in apposition are separated to allow each to heal independently.
The ideal substance is resorbable, adherent to the traumatized surface, applicable through the laparoscope, and inexpensive, with high biocompatibility. So far, no substance or material has proved to be unequivocally effective.
Adhesion barriers are widely studied
The following products are among the most widely investigated substances (TABLE 2).
Expanded polytetrafluoroethylene, or ePTFE. Gore-Tex surgical membrane, constructed of ePTFE (Preclude, WL Gore), is nonabsorbable and produced in thin sheets (0.1 mm), with an average pore size of less than 1 μm. It is sutured to the tissue so that it overlaps the incision by at least 1 cm. It prevents adhesion formation—and reformation—independent of the type of injury. It is also effective in the presence of blood.