KEY POINTS
- An extensive history is essential to identify the gravida at risk for a shortened cervical length.
- Transvaginal measurement of cervical lengths less than 26 mm has a high predictive value for preterm delivery.
- Prophylactic cerclage should be offered to patients with a classic history of cervical incompetence.
- The benefits of therapeutic cerclage for a shortened cervix remain uncertain, especially in women deemed to have a low risk of preterm delivery.
You are in your busy office, running behind schedule, when you receive a frantic notice from the ultrasound department that your patient—a primigravida scheduled for a routine anatomy survey at 21 weeks’ gestation—has a cervical length of 19 mm with funneling. What are your management options if the patient reports no contractions or changes in vaginal discharge?
With today’s emphasis on evidence-based medicine, it often is difficult to decide on an appropriate course of action, especially when conflicting reports abound. This article reviews the best studies available and presents a practical algorithm (FIGURE 1) to guide management of this difficult dilemma.
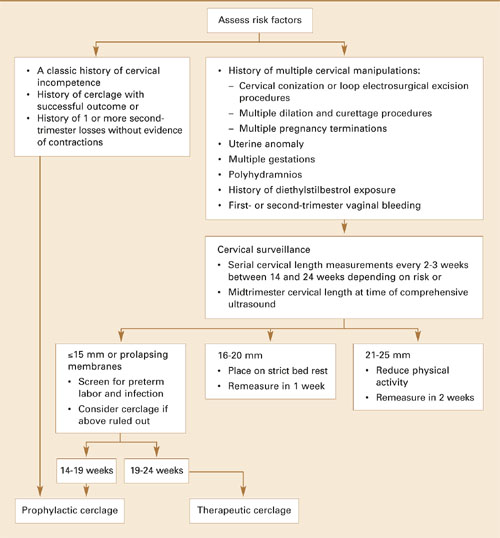
FIGURE 1 Management strategy for women with risk factors for cervical incompetence, preterm delivery
Predicting the need for cerclage
Despite numerous explorations of its pathophysiology, no irrefutable data explain what triggers the cascade of events leading to preterm birth, which remains a leading cause of morbidity and mortality. Cervical incompetence has been studied extensively as a possible cause, often without conclusive results.
Traditionally, cervical incompetence is defined as dilatation in the absence of contractions, usually presenting in the second trimester.1 Possible causes include prior obstetric or gynecologic injury, increased uterine volume (ie, multiple gestation, polyhydramnios), biological variation, and—currently under investigation—response to inflammatory mediators.2
In gravidas deemed to have biological or structural cervical incompetence, prophylactic cerclage is often placed at 12 to 14 weeks’ gestation. Alternatively, a therapeutic or “rescue” cerclage sometimes is placed at 20 weeks or more when evidence of cervical shortening or funneling is noted incidentally on ultrasound examination. At times, therapeutic cerclage becomes an emergency if prolapsing membranes are found.
With improvements in ultrasound imaging, transvaginal measurement of cervical length has become useful for guiding decisions on the need for cerclage.3,4 Unfortunately, current studies report conflicting data on the outcomes of pregnancies managed with cerclage placement based on ultrasound imaging.5-7
Ultrasound evaluation: Cervical length and other variables
In unselected general obstetric populations, preterm birth is associated with decreasing cervical length not only at 24 and 28 weeks’ gestation, but as early as 16 to 22 weeks’ gestation.8-14 Decreasing cervical length also predicts preterm birth in women at risk for early delivery.15,16 As a result, sonographic visualization of cervical length has evolved into a common practice to help predict early delivery.
An extensive history may offer clues as to what may have caused a shortened cervix in a previous pregnancy.
Iams et al17 compared cervical length with fetal fibronectin and noted that cervical length is more sensitive (39% versus 23%) but has a lower positive predictive value (PPV) (14% versus 20%). In combination, the modalities improved PPV to 50%. However, a separate study by Heath et al18 suggested that women with a cervical length of 15 mm or less had a relative risk of preterm birth 6 times greater than those with positive fetal fibronectin alone.
As sonographic technology has advanced, cervical characteristics have been assessed in a variety of ways. Besides measuring cervical length, experts also look for funneling, dilatation, prolapsing membranes, and dynamic changes elicited with transfundal or suprapubic pressure.4,19,20
Although cervical length can be measured transabdominally and transperineally, transvaginal assessment is most accurate. Transvaginal measurements also are more predictive and reproducible than traditional digital cervical examinations.16,21,22
Basic parameters. Standard cervical measurements use the “white stripe” of the internal cervical os as an anatomic landmark for proper caliper placement (FIGURE 2). As for dimensions of the nonlaboring cervix, Anderson23 found an average length of 45±7 mm at 14 to 30 weeks, and Iams et al10 found a mean cervical length of 35±8 mm at 24 weeks’ gestation after studying more than 2,900 gravidas. In another investigation, Hibbard and colleagues found a mean cervical length of 38.5±8 mm at 20 weeks’ gestation.12
Cervical length and diameter should remain constant as gestation progresses in both primiparous and multiparous women.22
Defining the short cervix. In a multicenter clinical trial, Iams et al10 measured the length of the cervix at 24 and 28 weeks in an unselected gravid population and determined that a length less than 26 mm at 24 weeks increases the relative risk for preterm delivery by a factor of 6.19, with a sensitivity of 37% for delivery before 35 weeks and a PPV of 18%—thus establishing the definition of a short cervix.